
Search
- Page Path
- HOME > Search
Original Articles
- Clinical Study
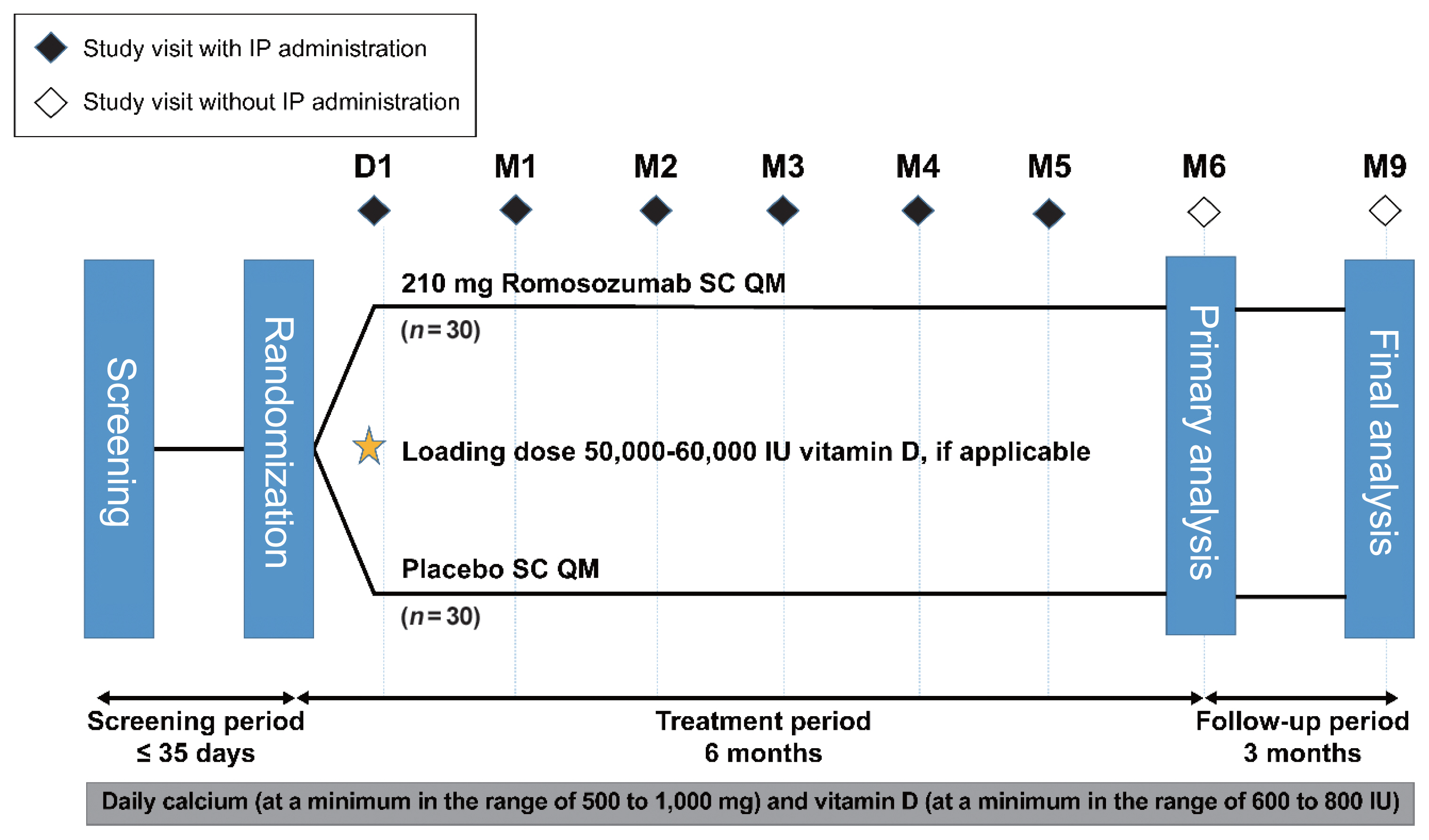
- Romosozumab in Postmenopausal Korean Women with Osteoporosis: A Randomized, Double-Blind, Placebo-Controlled Efficacy and Safety Study
- Ki-Hyun Baek, Yoon-Sok Chung, Jung-Min Koh, In Joo Kim, Kyoung Min Kim, Yong-Ki Min, Ki Deok Park, Rajani Dinavahi, Judy Maddox, Wenjing Yang, Sooa Kim, Sang Jin Lee, Hyungjin Cho, Sung-Kil Lim
- Endocrinol Metab. 2021;36(1):60-69. Published online February 24, 2021
- DOI: https://doi.org/10.3803/EnM.2020.848
- 6,790 View
- 390 Download
- 7 Web of Science
- 10 Crossref
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material PubReader
PubReader  ePub
ePub - Background
This phase 3 study evaluated the efficacy and safety of 6-month treatment with romosozumab in Korean postmenopausal women with osteoporosis.
Methods
Sixty-seven postmenopausal women with osteoporosis (bone mineral density [BMD] T-scores ≤–2.5 at the lumbar spine, total hip, or femoral neck) were randomized (1:1) to receive monthly subcutaneous injections of romosozumab (210 mg; n=34) or placebo (n=33) for 6 months.
Results
At month 6, the difference in the least square (LS) mean percent change from baseline in lumbar spine BMD (primary efficacy endpoint) between the romosozumab (9.5%) and placebo (–0.1%) groups was significant (9.6%; 95% confidence interval, 7.6 to 11.5; P<0.001). The difference in the LS mean percent change from baseline was also significant for total hip and femoral neck BMD (secondary efficacy endpoints). After treatment with romosozumab, the percent change from baseline in procollagen type 1 N-terminal propeptide transiently increased at months 1 and 3, while that in C-terminal telopeptide of type 1 collagen showed a sustained decrease. No events of cancer, hypocalcemia, injection site reaction, positively adjudicated atypical femoral fracture or osteonecrosis of the jaw, or positively adjudicated serious cardiovascular adverse events were observed. At month 9, 17.6% and 2.9% of patients in the romosozumab group developed binding and neutralizing antibodies, respectively.
Conclusion
Treatment with romosozumab for 6 months was well tolerated and significantly increased lumbar spine, total hip, and femoral neck BMD compared with placebo in Korean postmenopausal women with osteoporosis (ClinicalTrials.gov identifier NCT02791516). -
Citations
Citations to this article as recorded by
- A pharmacovigilance analysis of FDA adverse event reporting system events for romosozumab
Zepeng Chen, Ming Li, Shuzhen Li, Yuxi Li, Junyan Wu, Kaifeng Qiu, Xiaoxia Yu, Lin Huang, Guanghui Chen
Expert Opinion on Drug Safety.2023; 22(4): 339. CrossRef - Evaluation of the efficacy and safety of romosozumab (evenity) for the treatment of osteoporotic vertebral compression fracture in postmenopausal women: A systematic review and meta‐analysis of randomized controlled trials (CDM‐J)
Wenbo Huang, Masashi Nagao, Naohiro Yonemoto, Sen Guo, Takeshi Tanigawa, Yuji Nishizaki
Pharmacoepidemiology and Drug Safety.2023; 32(6): 671. CrossRef - Efficacy and Cardiovascular Safety of Romosozumab: A Meta-analysis and Systematic Review
Seo-Yong Choi, Jeong-Min Kim, Sang-Hyeon Oh, Seunghyun Cheon, Jee-Eun Chung
Korean Journal of Clinical Pharmacy.2023; 33(2): 128. CrossRef - Clinical Studies On Romosozumab: An Alternative For Individuals With A High Risk Of Osteoporotic Fractures: A Current Concepts Review (Part I)
E. Carlos Rodriguez-Merchan, Alonso Moreno-Garcia, Hortensia De la Corte-Rodriguez
SurgiColl.2023;[Epub] CrossRef - Romosozumab in osteoporosis: yesterday, today and tomorrow
Dong Wu, Lei Li, Zhun Wen, Guangbin Wang
Journal of Translational Medicine.2023;[Epub] CrossRef - Efficacy and safety of anti-sclerostin antibodies in the treatment of osteoporosis: A meta-analysis and systematic review
Frideriki Poutoglidou, Efthimios Samoladas, Nikolaos Raikos, Dimitrios Kouvelas
Journal of Clinical Densitometry.2022; 25(3): 401. CrossRef - Benefits of lumican on human bone health: clinical evidence using bone marrow aspirates
Yun Sun Lee, So Jeong Park, Jin Young Lee, Eunah Choi, Beom-Jun Kim
The Korean Journal of Internal Medicine.2022; 37(4): 821. CrossRef - What is the risk of cardiovascular events in osteoporotic patients treated with romosozumab?
I. R. Reid
Expert Opinion on Drug Safety.2022; 21(12): 1441. CrossRef - Proxied Therapeutic Inhibition on Wnt Signaling Antagonists and Risk of Cardiovascular Diseases: Multi-Omics Analyses
Yu Qian, Cheng-Da Yuan, Saber Khederzadeh, Ming-Yu Han, Hai-Xia Liu, Mo-Chang Qiu, Jian-Hua Gao, Wei-Lin Wang, Yun-Piao Hou, Guo-Bo Chen, Ke-Qi Liu, Lin Xu, David Karasik, Shu-Yang Xie, Hou-Feng Zheng
SSRN Electronic Journal .2022;[Epub] CrossRef - Multi-Omics Analyses Identify Pleiotropy and Causality Between Circulating Sclerostin and Atrial Fibrillation
Yu Qian, Peng-Lin Guan, Saber Khederzadeh, Ke-Qi Liu, Cheng-Da Yuan, Ming-Yu Han, Hai-Xia Liu, Mo-Chang Qiu, Jian-Hua Gao, Wei-Lin Wang, Yun-Piao Hou, Guo-Bo Chen, Lin Xu, David Karasik, Shu-Yang Xie, sheng zhifeng, Hou-Feng Zheng
SSRN Electronic Journal .2022;[Epub] CrossRef
- A pharmacovigilance analysis of FDA adverse event reporting system events for romosozumab

- Clinical Study
- Effects of Single Vitamin D3 Injection (200,000 Units) on Serum Fibroblast Growth Factor 23 and Sclerostin Levels in Subjects with Vitamin D Deficiency
- Dongdong Zhang, Da Hea Seo, Han Seok Choi, Hye-Sun Park, Yoon-Sok Chung, Sung-Kil Lim
- Endocrinol Metab. 2017;32(4):451-459. Published online December 14, 2017
- DOI: https://doi.org/10.3803/EnM.2017.32.4.451
- 4,556 View
- 50 Download
- 8 Web of Science
- 10 Crossref
-
Abstract
PDFPubReader
Background Vitamin D deficiency remains common in all age groups and affects skeletal and non-skeletal health. Fibroblast growth factor 23 is a bone-derived hormone that regulates phosphate and 1,25-dihydroxyvitamin D homeostasis as a counter regulatory factor. 1,25-Dihydroxyvitamin D stimulates fibroblast growth factor 23 synthesis in bone, while fibroblast growth factor 23 suppresses 1,25-dihydroxyvitamin D production in the kidney. The aim of this study was to evaluate the effects of vitamin D3 intramuscular injection therapy on serum fibroblast growth factor 23 concentrations, and several other parameters associated with bone metabolism such as sclerostin, dickkopf-1, and parathyroid hormone.
Methods A total of 34 subjects with vitamin D deficiency (defined by serum 25-hydroxyvitamin D levels below 20 ng/mL) were randomly assigned to either the vitamin D injection group (200,000 units) or placebo treatment group. Serum calcium, phosphate, urine calcium/creatinine, serum 25-hydroxyvitamin D, fibroblast growth factor 23, sclerostin, parathyroid hormone, and dickkopf-1 levels were serially measured after treatment.
Results Comparing the vitamin D injection group with the placebo group, no significant changes were observed in serum fibroblast growth factor 23, parathyroid hormone, or dickkopf-1 levels. Serum sclerostin concentrations transiently increased at week 4 in the vitamin D group. However, these elevated levels declined later and there were no statistically significant differences as compared with baseline levels.
Conclusion Serum fibroblast factor 23, sclerostin, parathyroid hormone, and dickkopf-1 levels were not affected significantly by single intramuscular injection of vitamin D3.
-
Citations
Citations to this article as recorded by- Effect of vitamin D supplementation on circulating fibroblast growth factor-23 concentration in adults with prediabetes
Lisa Ceglia, Anastassios G. Pittas, Bess Dawson-Hughes
Aging Clinical and Experimental Research.2023; 35(3): 525. CrossRef - Fibroblast Growth Factor 23 in COVID-19: An Observational Study
Athena Myrou, Theodoros Aslanidis, Keli Makedou, Athanasios Mitsianis, Aikaterini Thisiadou, Paraskevi Karalazou, Georgios Chatzopoulos, Anastasios Papadopoulos, Antonios Kalis, Dimitrios Giagkoulis, Fotios Lezgidis, Christos Savopoulos
Cureus.2023;[Epub] CrossRef - The effect of vitamin D supplementation on serum levels of fibroblast growth factor- 23: A systematic review and meta-analysis of randomized controlled trials
Fatemeh Meshkini, Sepideh Soltani, Cain C.T. Clark, Vivian Tam, David Meyre, Omid Toupchian, Sahar Saraf-Bank, Shima Abdollahi
The Journal of Steroid Biochemistry and Molecular Biology.2022; 215: 106012. CrossRef - Serum sclerostin levels in osteoporotic fracture patients
Erwin A. Gorter, Casper R. Reinders, Pieta Krijnen, Natasha M. Appelman-Dijkstra, Inger B. Schipper
European Journal of Trauma and Emergency Surgery.2022; 48(6): 4857. CrossRef - Clinical Utility of Preoperative Vitamin D3 Injection for Preventing Transient Hypocalcemia after Total Thyroidectomy
Kwangsoon Kim, Cho Rok Lee, Sang-Wook Kang, Jandee Lee, Jong Ju Jeong, Kee-Hyun Nam, Woong Youn Chung, Claudio Casella
International Journal of Endocrinology.2021; 2021: 1. CrossRef - The effect of vitamin D supplementation on fibroblast growth factor‐23 in patients with chronic kidney disease: A systematic review and meta‐analysis
Elmira Karimi, Sama Bitarafan, Seyed Mohammad Mousavi, Nikan Zargarzadeh, Pari Mokhtari, Jessie Hawkins, Alipasha Meysamie, Fariba Koohdani
Phytotherapy Research.2021; 35(10): 5339. CrossRef - Pharmacodynamics of Oral Cholecalciferol in Healthy Individuals with Vitamin D Deficiency: A Randomized Open-Label Study
Angelo Fassio, Davide Gatti, Maurizio Rossini, Camilla Benini, Elena Fracassi, Eugenia Bertoldo, Ombretta Viapiana, Stefano Milleri, Matteo Gatti, Giovanni Adami
Nutrients.2021; 13(7): 2293. CrossRef - Vitamin D Deficiency at Mid-Pregnancy Is Associated with a Higher Risk of Postpartum Glucose Intolerance in Women with Gestational Diabetes Mellitus
Kyung-Soo Kim, Seok Won Park, Yong-Wook Cho, Soo-Kyung Kim
Endocrinology and Metabolism.2020; 35(1): 97. CrossRef - Effects of vitamin D supplementation on bone turnover markers and other bone-related substances in subjects with vitamin D deficiency
Rolf Jorde, Astrid Kamilla Stunes, Julia Kubiak, Ragnar Joakimsen, Guri Grimnes, Per Medbøe Thorsby, Unni Syversen
Bone.2019; 124: 7. CrossRef - Vitamin D Enhances the Efficacy of Topical Artificial Tears in Patients With Dry Eye Disease
Jin Sun Hwang, Yoon Pyo Lee, Young Joo Shin
Cornea.2019; 38(3): 304. CrossRef
- Effect of vitamin D supplementation on circulating fibroblast growth factor-23 concentration in adults with prediabetes
- Site-Specific Difference of Bone Geometry Indices in Hypoparathyroid Patients
- Hye-Sun Park, Da Hea Seo, Yumie Rhee, Sung-Kil Lim
- Endocrinol Metab. 2017;32(1):68-76. Published online February 6, 2017
- DOI: https://doi.org/10.3803/EnM.2017.32.1.68
- 3,306 View
- 32 Download
- 3 Web of Science
- 4 Crossref
-
Abstract
PDFPubReader
Background Hypoparathyroid patients often have a higher bone mineral density (BMD) than the general population. However, an increase in BMD does not necessarily correlate with a solid bone microstructure. This study aimed to evaluate the bone microstructure of hypoparathyroid patients by using hip structure analysis (HSA).
Methods Ninety-five hypoparathyroid patients >20 years old were enrolled and 31 of them had eligible data for analyzing bone geometry parameters using HSA. And among the control data, we extracted sex-, age-, and body mass index-matched three control subjects to each patient. The BMD data were reviewed retrospectively and the bone geometry parameters of the patients were analyzed by HSA.
Results The mean Z-scores of hypoparathyroid patients at the lumbar spine, femoral neck, and total hip were above zero (0.63±1.17, 0.48±1.13, and 0.62±1.10, respectively). The differences in bone geometric parameters were site specific. At the femoral neck and intertrochanter, the cross-sectional area (CSA) and cortical thickness (C.th) were higher, whereas the buckling ratio (BR) was lower than in controls. However, those trends were opposite at the femoral shaft; that is, the CSA and C.th were low and the BR was high.
Conclusion Our study shows the site-specific effects of hypoparathyroidism on the bone. Differences in bone components, marrow composition, or modeling based bone formation may explain these findings. However, further studies are warranted to investigate the mechanism, and its relation to fracture risk.
-
Citations
Citations to this article as recorded by- Vertebral fractures, trabecular bone score and their determinants in chronic hypoparathyroidism
S. Saha, V. Mannar, D. Kandasamy, V. Sreenivas, R. Goswami
Journal of Endocrinological Investigation.2022; 45(9): 1777. CrossRef - Epidemiology and Financial Burden of Adult Chronic Hypoparathyroidism
Sigridur Bjornsdottir, Steven Ing, Deborah M Mitchell, Tanja Sikjaer, Line Underbjerg, Zaki Hassan-Smith, Jad Sfeir, Neil J Gittoes, Bart L Clarke L
Journal of Bone and Mineral Research.2020; 37(12): 2602. CrossRef - Effect of Endogenous Parathyroid Hormone on Bone Geometry and Skeletal Microarchitecture
A Ram Hong, Ji Hyun Lee, Jung Hee Kim, Sang Wan Kim, Chan Soo Shin
Calcified Tissue International.2019; 104(4): 382. CrossRef - Bone responses to chronic treatment of adult hypoparathyroid patients with PTH peptides
Sofie Malmstroem, Lars Rejnmark, Dolores M. Shoback
Current Opinion in Endocrine and Metabolic Research.2018; 3: 51. CrossRef
- Vertebral fractures, trabecular bone score and their determinants in chronic hypoparathyroidism
- Endocrine Research
- The Role of Nuclear Factor-E2-Related Factor 1 in the Oxidative Stress Response in MC3T3-E1 Osteoblastic Cells
- So Young Park, Sung Hoon Kim, Hyun Koo Yoon, Chang Hoon Yim, Sung-Kil Lim
- Endocrinol Metab. 2016;31(2):336-342. Published online April 25, 2016
- DOI: https://doi.org/10.3803/EnM.2016.31.2.336
- 3,954 View
- 61 Download
- 10 Web of Science
- 9 Crossref
-
Abstract
PDFPubReader
Background Reactive oxygen species (ROS) and antioxidants are associated with maintenance of cellular function and metabolism. Nuclear factor-E2-related factor 1 (NFE2L1, Nrf1) is known to regulate the expression of a number of genes involved in oxidative stress and inflammation. The purpose of this study was to examine the effects of NFE2L1 on the response to oxidative stress in osteoblastic MC3T3-E1 cells.
Methods The murine calvaria-derived MC3T3-E1 cell line was exposed to lipopolysaccharide (LPS) for oxidative stress induction. NFE2L1 effects were evaluated using small interfering RNA (siRNA) for
NFE2L1 mRNA. ROS generation and the levels of known antioxidant enzyme genes were assayed.Results NFE2L1 expression was significantly increased 2.4-fold compared to the control group at 10 µg/mL LPS in MC3T3-E1 cells (P <0.05). LPS increased formation of intracellular ROS in MC3T3-E1 cells.NFE2L1 knockdown led to an additional increase of ROS (20%) in the group transfected withNFE2L1 siRNA compared with the control group under LPS stimulation (P <0.05). RNA interference ofNFE2L1 suppressed the expression of antioxidant genes including metallothionein 2, glutamatecysteine ligase catalytic subunit, and glutathione peroxidase 1 in LPS-treated MC3T3-E1 cells.Conclusion Our results suggest that NFE2L1 may have a distinct role in the regulation of antioxidant enzymes under inflammation-induced oxidative stress in MC3T3-E1 osteoblastic cells.
-
Citations
Citations to this article as recorded by- SDH5 down-regulation mitigates the damage of osteoporosis via inhibiting the MyD88/NF-κB signaling pathway
Hongzi Wu, Dehua Zhang, Haijun Xia, Yongqi Li, Feng Mao, Yi Liao
Immunopharmacology and Immunotoxicology.2023; 45(3): 317. CrossRef - N-acetyl Cysteine Inhibits Cell Proliferation and Differentiation of LPSInduced MC3T3-E1 Cells Via Regulating Inflammatory Cytokines
Wangyang Li, Hui Zhang, Junchi Chen, Yujie Tan, Ailing Li, Ling Guo
Current Pharmaceutical Biotechnology.2023; 24(3): 450. CrossRef - Unravelling the role of NFE2L1 in stress responses and related diseases
Xingzhu Liu, Chang Xu, Wanglong Xiao, Nianlong Yan
Redox Biology.2023; 65: 102819. CrossRef - Nfe2l1 deficiency mitigates streptozotocin-induced pancreatic β-cell destruction and development of diabetes in male mice
Simeng Bao, Hongzhi Zheng, Chengjie Chen, Yuhang Zhang, Lina Bao, Bei Yang, Yongyong Hou, Yanyan Chen, Qiang Zhang, Jingbo Pi, Jingqi Fu
Food and Chemical Toxicology.2021; 158: 112633. CrossRef - Long isoforms of NRF1 negatively regulate adipogenesis via suppression of PPARγ expression
Peng Xue, Yongyong Hou, Zhuo Zuo, Zhendi Wang, Suping Ren, Jian Dong, Jingqi Fu, Huihui Wang, Melvin E. Andersen, Qiang Zhang, Yuanyuan Xu, Jingbo Pi
Redox Biology.2020; 30: 101414. CrossRef - Protracted rosiglitazone treatment exacerbates inflammation in white adipose tissues of adipocyte-specific Nfe2l1 knockout mice
Suping Ren, Yongyong Hou, Zhuo Zuo, Zhiyuan Liu, Huihui Wang, Yuanyuan Xu, Masayuki Yamamoto, Qiang Zhang, Jingqi Fu, Jingbo Pi
Food and Chemical Toxicology.2020; 146: 111836. CrossRef - Nrf1 is paved as a new strategic avenue to prevent and treat cancer, neurodegenerative and other diseases
Jianxin Yuan, Shuwei Zhang, Yiguo Zhang
Toxicology and Applied Pharmacology.2018; 360: 273. CrossRef - Silencing of long isoforms of nuclear factor erythroid 2 like 1 primes macrophages towards M1 polarization
Huihui Wang, Jiayu Zhu, Zhiyuan Liu, Hang Lv, Peng Lv, Feng Chen, Jingqi Fu, Yongyong Hou, Rui Zhao, Yuanyuan Xu, Qiang Zhang, Jingbo Pi
Free Radical Biology and Medicine.2018; 117: 37. CrossRef - Costunolide increases osteoblast differentiation via ATF4-dependent HO-1 expression in C3H10T1/2 cells
Wan-Jin Jeon, Kyeong-Min Kim, Eun-Jung Kim, Won-Gu Jang
Life Sciences.2017; 178: 94. CrossRef
- SDH5 down-regulation mitigates the damage of osteoporosis via inhibiting the MyD88/NF-κB signaling pathway
- Clinical Study
- Serum γ-Glutamyl Transferase Is Inversely Associated with Bone Mineral Density Independently of Alcohol Consumption
- Han Seok Choi, Kwang Joon Kim, Yumie Rhee, Sung-Kil Lim
- Endocrinol Metab. 2016;31(1):64-71. Published online March 16, 2016
- DOI: https://doi.org/10.3803/EnM.2016.31.1.64
- 4,187 View
- 37 Download
- 10 Web of Science
- 9 Crossref
-
Abstract
PDFPubReader
Background γ-Glutamyl transferase (GGT) is a well-known marker of chronic alcohol consumption or hepatobiliary diseases. A number of studies have demonstrated that serum levels of GGT are independently associated with cardiovascular and metabolic disorders. The purpose of this study was to test if serum GGT levels are associated with bone mineral density (BMD) in Korean adults.
Methods A total of 462 subjects (289 men and 173 women), who visited Severance Hospital for medical checkup, were included in this study. BMD was measured using dual energy X-ray absorptiometry. Cross-sectional association between serum GGT and BMD was evaluated.
Results As serum GGT levels increased from the lowest tertile (tertile 1) to the highest tertile (tertile 3), BMD decreased after adjusting for confounders such as age, body mass index, amount of alcohol consumed, smoking, regular exercise, postmenopausal state (in women), hypertension, diabetes mellitus, and hypercholesterolemia. A multiple linear regression analysis showed a negative association between log-transformed serum GGT levels and BMD. In a multiple logistic regression analysis, tertile 3 of serum GGT level was associated with an increased risk for low bone mass compared to tertile 1 (odds ratio, 2.271; 95% confidence interval, 1.340 to 3.850;
P =0.002).Conclusion Serum GGT level was inversely associated with BMD in Korean adults. Further study is necessary to fully elucidate the mechanism of the inverse relationship.
-
Citations
Citations to this article as recorded by- Association of gamma-glutamyl transferase variability with risk of osteoporotic fractures: A nationwide cohort study
Dongyeop Kim, Jee Hyun Kim, Heajung Lee, Iksun Hong, Yoonkyung Chang, Tae-Jin Song, Mohamed El-Sayed Abdel-Wanis
PLOS ONE.2023; 18(6): e0277452. CrossRef - Gamma-glutamyl-transferase is associated with incident hip fractures in women and men ≥ 50 years: a large population-based cohort study
W. Brozek, H. Ulmer, A. Pompella, G. Nagel, A. Leiherer, O. Preyer, H. Concin, E. Zitt
Osteoporosis International.2022; 33(6): 1295. CrossRef - Elevated gamma-glutamyl transpeptidase level is associated with an increased risk of hip fracture in postmenopausal women
Kyoung Jin Kim, Namki Hong, Min Heui Yu, Seunghyun Lee, Sungjae Shin, Sin Gon Kim, Yumie Rhee
Scientific Reports.2022;[Epub] CrossRef - Elevated serum γ-glutamyl transferase is associated with low muscle function in adults independent of muscle mass
Seunghyun Lee, Dawon Song, Sungjae Shin, Namki Hong, Yumie Rhee
Nutrition.2022; 103-104: 111813. CrossRef - A fluorine-18 labeled radiotracer for PET imaging of γ-glutamyltranspeptidase in living subjects
Dingyao Gao, Yinxing Miao, Siqin Ye, Chunmei Lu, Gaochao Lv, Ke Li, Chunjing Yu, Jianguo Lin, Ling Qiu
RSC Advances.2021; 11(31): 18738. CrossRef - The dark side of gamma-glutamyltransferase (GGT): Pathogenic effects of an ‘antioxidant’ enzyme
Alessandro Corti, Eugenia Belcastro, Silvia Dominici, Emilia Maellaro, Alfonso Pompella
Free Radical Biology and Medicine.2020; 160: 807. CrossRef - Clinical and body composition predictors of bone turnover and mineral content in obese postmenopausal women
Rim Cherif, Feten Mahjoub, Hela Sahli, Elhem Cheour, Mohsen Sakly, Nebil Attia
Clinical Rheumatology.2019; 38(3): 739. CrossRef - Association between liver enzymes and bone mineral density in Koreans: a cross-sectional study
Ho Jeong Do, Joon-Shik Shin, Jinho Lee, Yoon Jae Lee, Me-riong Kim, Dongwoo Nam, Eun-Jung Kim, Yeoncheol Park, Kristin Suhr, In-Hyuk Ha
BMC Musculoskeletal Disorders.2018;[Epub] CrossRef - Articles inEndocrinology and Metabolismin 2016
Won-Young Lee
Endocrinology and Metabolism.2017; 32(1): 62. CrossRef
- Association of gamma-glutamyl transferase variability with risk of osteoporotic fractures: A nationwide cohort study
- Bone Metabolism
- Increased Sclerostin Levels after Further Ablation of Remnant Estrogen by Aromatase Inhibitors
- Wonjin Kim, Yoonjung Chung, Se Hwa Kim, Sehee Park, Jae Hyun Bae, Gyuri Kim, Su Jin Lee, Jo Eun Kim, Byeong-Woo Park, Sung-Kil Lim, Yumie Rhee
- Endocrinol Metab. 2015;30(1):58-64. Published online March 27, 2015
- DOI: https://doi.org/10.3803/EnM.2015.30.1.58
- 4,089 View
- 36 Download
- 14 Web of Science
- 14 Crossref
-
Abstract
PDFPubReader
Background Sclerostin is a secreted Wnt inhibitor produced almost exclusively by osteocytes, which inhibits bone formation. Aromatase inhibitors (AIs), which reduce the conversion of steroids to estrogen, are used to treat endocrine-responsive breast cancer. As AIs lower estrogen levels, they increase bone turnover and lower bone mass. We analyzed changes in serum sclerostin levels in Korean women with breast cancer who were treated with an AI.
Methods We included postmenopausal women with endocrine-responsive breast cancer (
n =90; mean age, 57.7 years) treated with an AI, and compared them to healthy premenopausal women (n =36; mean age, 28.0 years). The subjects were randomly assigned to take either 5 mg alendronate with 0.5 µg calcitriol (n =46), or placebo (n =44) for 6 months.Results Postmenopausal women with breast cancer had significantly higher sclerostin levels compared to those in premenopausal women (27.8±13.6 pmol/L vs. 23.1±4.8 pmol/L,
P <0.05). Baseline sclerostin levels positively correlated with either lumbar spine or total hip bone mineral density only in postmenopausal women (r =0.218 andr =0.233;P <0.05, respectively). Serum sclerostin levels increased by 39.9%±10.2% 6 months after AI use in postmenopausal women; however, no difference was observed between the alendronate and placebo groups (39.9%±10.2% vs. 55.9%±9.13%,P >0.05).Conclusion Serum sclerostin levels increased with absolute deficiency of residual estrogens in postmenopausal women with endocrine-responsive breast cancer who underwent AI therapy with concurrent bone loss.
-
Citations
Citations to this article as recorded by- Voluntary Wheel Running Partially Compensates for the Effects of Global Estrogen Receptor-α Knockout on Cortical Bone in Young Male Mice
Rebecca K. Dirkes, Nathan C. Winn, Thomas J. Jurrissen, Dennis B. Lubahn, Victoria J. Vieira-Potter, Jaume Padilla, Pamela S. Hinton
International Journal of Molecular Sciences.2021; 22(4): 1734. CrossRef - Role of Osteocytes in Cancer Progression in the Bone and the Associated Skeletal Disease
Manish Adhikari, Jesús Delgado-Calle
Current Osteoporosis Reports.2021; 19(3): 247. CrossRef - Gestational and lactational exposure to BPA or BPS has minimal effects on skeletal outcomes in adult female mice
Rebecca K. Dirkes, Rebecca J. Welly, Jiude Mao, Jessica Kinkade, Victoria J. Vieira-Potter, Cheryl S. Rosenfeld, Pamela S. Bruzina
Bone Reports.2021; 15: 101136. CrossRef - Modulation of bone turnover aberration: A target for management of primary osteoporosis in experimental rat model
Enas A. Fouad-Elhady, Hadeer A. Aglan, Rasha E. Hassan, Hanaa H. Ahmed, Gilane M. Sabry
Heliyon.2020; 6(2): e03341. CrossRef - Aromatase inhibitors attenuate the effect of alendronate in women with breast cancer
Sung Hye Kong, Jung Hee Kim, Sang Wan Kim, Chan Soo Shin
Journal of Bone and Mineral Metabolism.2020; 38(5): 730. CrossRef - Global estrogen receptor-α knockout has differential effects on cortical and cancellous bone in aged male mice
Rebecca K. Dirkes, Nathan C. Winn, Thomas J. Jurrissen, Dennis B. Lubahn, Victoria J. Vieira-Potter, Jaume Padilla, Pamela S. Hinton, Vance L. Trudeau
FACETS.2020; 5(1): 328. CrossRef - The Emerging Role of Osteocytes in Cancer in Bone
Emily G Atkinson, Jesús Delgado‐Calle
JBMR Plus.2019;[Epub] CrossRef - Effect of denosumab on low bone mineral density in postmenopausal Japanese women receiving adjuvant aromatase inhibitors for non-metastatic breast cancer: 24-month results
Katsuhiko Nakatsukasa, Hiroshi Koyama, Yoshimi Ouchi, Hisako Ono, Kouichi Sakaguchi, Takayuki Matsuda, Makoto Kato, Takashi Ishikawa, Kimito Yamada, Mana Yoshimura, Kei Koizumi, Teruhisa Sakurai, Hideo Shigematsu, Shunji Takahashi, Shinichiro Taira, Masat
Breast Cancer.2019; 26(1): 106. CrossRef - Association of Wnt Inhibitors, Bone Mineral Density and Lifestyle Parameters in Women with Breast Cancer Treated with Anastrozole Therapy
Kristina Bojanić, Ines Bilić Ćurčić, Lucija Kuna, Tomislav Kizivat, Robert Smolic, Nikola Raguž Lučić, Kristina Kralik, Vatroslav Šerić, Gordana Ivanac, Sandra Tucak-Zorić, Aleksandar Včev, Martina Smolić
Journal of Clinical Medicine.2018; 7(9): 287. CrossRef - Management of Aromatase Inhibitor-Associated Bone Loss (AIBL) in postmenopausal women with hormone sensitive breast cancer: Joint position statement of the IOF, CABS, ECTS, IEG, ESCEO, IMS, and SIOG
Peyman Hadji, Matti S. Aapro, Jean-Jacques Body, Michael Gnant, Maria Luisa Brandi, Jean Yves Reginster, M. Carola Zillikens, Claus-C. Glüer, Tobie de Villiers, Rod Baber, G. David Roodman, Cyrus Cooper, Bente Langdahl, Santiago Palacios, John Kanis, Nass
Journal of Bone Oncology.2017; 7: 1. CrossRef - Effects of raloxifene against letrozole-induced bone loss in chemically-induced model of menopause in mice
Abul Kalam, Sushama Talegaonkar, Divya Vohora
Molecular and Cellular Endocrinology.2017; 440: 34. CrossRef - Sclerostin: an Emerging Target for the Treatment of Cancer-Induced Bone Disease
Michelle M. McDonald, Jesus Delgado-Calle
Current Osteoporosis Reports.2017; 15(6): 532. CrossRef - Differential profile of letrozole and exemestane on bone turnover markers in vinylcyclohexene diepoxide treated ovotoxic female mice
Abul Kalam, Sushama Talegaonkar, Divya Vohora
Fundamental & Clinical Pharmacology.2016; 30(5): 429. CrossRef - Osteoblasts Are the Centerpiece of the Metastatic Bone Microenvironment
Hyo Min Jeong, Sun Wook Cho, Serk In Park
Endocrinology and Metabolism.2016; 31(4): 485. CrossRef
- Voluntary Wheel Running Partially Compensates for the Effects of Global Estrogen Receptor-α Knockout on Cortical Bone in Young Male Mice
 First
First Prev
Prev


